
Innovative Best Practice Models of Care
Bridges and Pathways works to present solutions and to bridge the gaps in healthcare for Australians living with poorly understood complex chronic conditions, working from current best practice towards evidence-based care.
Australians Need Services Now: While there are no definitive diagnostic tests or approved treatments for ME/CFS or Fibromyalgia, there are many effective interventions that improve quality of life and significantly reduce symptom burden.
The Australian ME/CFS/FMS Best Practice Primary Care Service Models outlined are based on the findings from a series of collaborative research service improvement projects (2002-2025). They are informed by key documents and evolving biomedical research.
These projects are part of Australian health care reforms, including General Practice Enhanced Primary Care, Chronic Disease Management education and referrals, pathways of care, early diagnosis, provider and consumer education, as well as expanding to flexible modes for more effective delivery (Telehealth and digital platforms).
Bridges & Pathways participated to represent the 500,000+ Australians living with ME/CFS (Myalgic Encephalomyelitis /Chronic Fatigue Syndrome) and Fibromyalgia (60-90% overlap). Our aim is to have these non-priority conditions included in health service delivery, specifically to ensure ‘equal access to medical care for Australians living with these poorly understood conditions’.
The project work has involved consultations with clinicians, patients and other stakeholders; focus groups, surveys, and service outcome surveys.
Stakeholders have identified programs from wider health services that can be applied to improve services in real life settings.
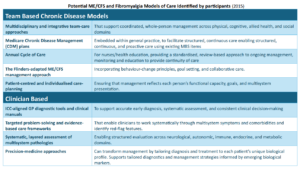
Adaptation of Broader Health Programs
The project steering groups have examined established programs across wider health services and adapted them to improve ME/CFS and Fibromyalgia care in real-world settings. This work ensures that proven approaches, such as chronic-disease frameworks, self-management programs, care-coordination systems, and primary-care assessment tools, are modified to address the specific needs, risks, and multisystem presentations of ME/CFS and Fibromyalgia.
The resulting programs are being developed into tailored pathways of care (models of care) to improve the diagnosis, early intervention and management, while identifying and addressing the barriers to providing and receiving appropriate health care for Australians. They provide immediate cost-effective frameworks for health services to deliver patient-centred, multi-disciplinary and wellness focussed care.
The different models of care outline systematic best practice care and service delivery for this patient cohort as they progress through the stages of their condition. They are consistent with current Medicare chronic disease management team care, as well as the changes being promoted as part of the National Strategic Framework for Chronic Conditions, 2017.
For Australians with complex multisystem multifactorial conditions (now including long COVID), the models provide best practice systematic care and referral pathways to address the multiple issues in providing care and limiting hospital admissions. For Australian General Practice referral networks, they provide early diagnosis, standardised assessments and tailored management care pathways and referral protocols.
1. SOUTH AUSTRALIAN NURSE-LED, GP-EMBEDDED EARLY DIAGNOSIS SCREENING & MANAGEMENT MODEL (2024)
Many Australians living with ME/CFS and Fibromyalgia (60-90% overlap) face long delays (average 4-7 years) before receiving a diagnosis. There are long waiting lists for specialist clinics.
Missed or delayed diagnoses can lead to further functional decline, limited access to support services, and reduced quality of life. It also places strain on GPs, who are left to manage patients with persistent, unexplained symptoms without clear clinical pathways or specialist referral options.
Our research found nurses are an under-recognised workforce, despite routinely delivering Medicare Chronic Disease Management care plans, monitoring symptoms and functional assessments in general practice, as well as conducting pre-consultation screening in hospital and other specialist clinics, roles that improve efficiency and reduce pressure on medical services.
The Nurse-Led, GP-Embedded Early Diagnostic Screening & Management Model operates as an extension of Medicare Chronic Disease Management by embedding ME/CFS and Fibromyalgia-specific assessment tools, structured cycle-of-care processes and multidisciplinary communication into standard GP workflows.
These tools include:
- Standardised diagnostic screening instruments aligned with international criteria (e.g. ME/CFS ICC-based screens and Fibromyalgia Symptom Questionnaires)
- Post-exertional malaise (PEM) assessment tools to identify hallmark disease features and guide safe management
- Functional and symptom severity measures to monitor disability, daily functioning and clinical change over time
- Autonomic and orthostatic screening, such as the NASA Lean Test
- Structured documentation templates integrated with Medicare Care Plans, Annual Reviews, and GP software systems to enable coordinated multidisciplinary management, referrals and reporting.
A 2024 ‘proof of concept’ study found that the diagnostic screening and assessment process facilitated more focussed consultations, enhanced the diagnostic experience and set a strong foundation for ongoing shared management. Patients valued the staged approach, nurse-led consultations, and the sense of being heard & validated.
This model provides a scalable, cost-effective solution that enhances the capacity of general practice, improves diagnostic confidence, and supports proactive management from the earliest stages of presentation.
The work continues to evolve, subject to the availability of funding, as part of a larger multi-agency initiative to reduce waiting times for specialist clinics (2025-26) and to streamline primary-care referrals, with nurses and medical students providing early diagnostic screening and appropriate referrals for Australians living with ME/CFS and Fibromyalgia.
2. GENERAL PRACTICE CARE PATHWAYS CLINICAL NETWORK MODEL (2021)
This model of care is a further development of our Australian ME/CFS/FMS Best Practice General Practice Care (2016) model (see below). There are ongoing barriers to medical care, frustrating both patients and their providers. Many patients still report they have attended multiple providers before being diagnosed or accessing appropriate treatments. This has increased since Covid and with the current shortage of General Practitioners and the closure of many hospital clinics. This causes further burden on the health system as patients struggle to find providers who will provide documentation for Centrelink and NDIS.
The clinical pathways model of care has been extended to use General Practice based treatment algorithms (Health Pathways) and assessment tools to support the documentation requirements for Australian Centrelink and the National Disability Insurance Scheme. The final assessments in the model were developed in consultation with disability case managers and advocates to address the current barriers for inclusion into disability and welfare services.
This clinical pathways model continues to evolve based on feedback from participating clinics and consumers and the coming Australian NHMRC Guidelines.
3. AUSTRALIAN ME/CFS/FMS BEST PRACTICE GENERAL PRACTICE CARE (2016)
This General Practice based model of care was developed to address delays in diagnosis and management. Clients were reporting that they could not find doctors to confirm their diagnosis, and some were presenting with the wrong diagnosis. Delays in diagnosis meant patients were becoming unnecessarily disabled and dependent on health and welfare. The model uses a targeted stepwise problem-solving approach with standardised assessment tools to support diagnosis and management.
The Model of Care process includes:
- An accurate diagnosis (using standard questionnaires; may take several visits).
- Best practice ME/CFS or Fibromyalgia medical care tailored for each patient. It includes:
- Early intervention
- Layered Comprehensive Assessments to guide management and treatment pathways
- Targeted problem solving
- Tailored patient-centred care planning and case management
- Health education and coaching to support shared care.
- Annual care planning and reviews (Medicare CDMP Items 721, 723, 731, 732) that focus on patient outcomes and detailed health care needs, services and treatments for the coming year, and lists of what the person needs to do.
- Referrals to allied health professionals who understand the pathophysiology of each patient’s condition e.g. exercise therapist, dietitian, psychologist, and physiotherapist.
- Regular reviews of care and health outcomes with adjustments based on patient feedback and medical outcomes towards optimal management.
4. THE AUSTRALIAN BEST PRACTICE ME/CFS/FMS INTEGRATED EDUCATION MODEL (2012)
This Model of Care contains 8 components or essential core steps consistent with the Flinders Chronic Disease Management Program. It provides a framework to assess/incorporate wider Chronic Disease Management Education programs into ME/CFS and Fibromyalgia management plans and pathways of care. These multi-disciplinary programs are delivered via multiple platforms including online, Telehealth, and digital platforms.
Essential Core Steps include:
- Have knowledge of ME/CFS/FMS and management options
- Have a treatment and care plan to coordinate a healthcare team
- Actively share in decision making with the healthcare team
- Monitor and manage the signs and symptoms of ME/CFS and Fibromyalgia
- Manage ME/CFS/FMS using a mixture of medical and lifestyle decisions (physical, mental, emotional and social life)
- Adopt a lifestyle that promotes health (sleep, stress, diet and movement)
- Extend the care plan to use education, community and other support services
- Regularly review the care in partnership with case manager.
Shared care in this Model is supported by an Annual Cycle of Care Program, checklists and patient information resources (2015).
5. The AUSTRALIAN ME/CFS/FMS BEST PRACTICE CARE PATHWAYS SERVICE MODELS (2008)
Our first Models of Care were developed working with Medicare Locals and projects, implementing ‘Enhanced Primary Care’ and Stanford Chronic Disease Self-Management Education Programs. People completing the patient education programs were unable to find services to support their proactive self-management. In turn practice nurses and general practitioners had no information to develop enhanced primary care /chronic disease management care planning and referrals.
The Model of Care includes:
- Comprehensive Assessments and an accurate diagnosis (based on Canadian Clinical Guidelines)
- Health Care planning and referrals to allied health and community programs coordinated and monitored by a Medicare Chronic Disease Management framework
- Best practice medical care tailored for each patient:
- Early intervention including recommendations on pacing and trying new treatments using the start low go slow method
- Layered targeted problem-solving approach to clinical presentation
- Tailored patient-centred care planning incorporating life stage and community supports
- Documenting all multi-disciplinary, interventions, allied health / health related services into care plans and stressing the ‘introduce one at a time, on a start low / go slow method’.
- Patients are encouraged to be proactive and self-monitor
- Patient feedback is incorporated into assessments and management decisions.
The South Australian ME/CFS/FMS Clinical Research Collaboration Projects are working continually to provide current best practice services and programs for all Australians.
We welcome your suggestions and input. Please Contact Us.