
Diagnosis
General Practice Diagnosis
Primary Symptom
Additional Symptoms
ME/CFS diagnosis is based on a detailed clinical history, physical examination, and laboratory investigations. While symptoms vary from patient to patient there are standard criteria to aid a clinical diagnosis – International ME/CFS Primer, 2014
Useful clinical tools / questionnaires include:
- International (IACFSME) ME/CFS Clinical Criteria – Simplified Checklist for Australian GP Clinics (2024 update)
- IACFSME Primer 2014: Pediatric ME/CFS Case Definition Worksheet
- Fibromyalgia Screening Questionnaire (FSQ) (Hauser et al., 2012) – simpler tool useful for quantifying symptoms for care planning
- PEM Screening Worksheet (Bateman Horne)
- PEM DePaul University DSQ-PEM (Jason)
Download Assessment Tools here
Understanding the Diagnostic Process
The hallmark of ME/CFS is post exertional malaise (PEM), the failure to recover after physical or mental activities. In a clinical setting this may be interpreted as a physical fatigue which needs to be investigated.
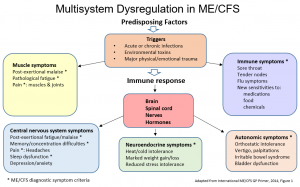
The International Primer describes ME/CFS as having Multisystem Dysregulation that presents as an array of seemingly unrelated symptoms. For more information on the symptoms see below.
General Practice Diagnosis
Accurate diagnosis requires a comprehensive assessment of symptoms, contributing factors, and potential underlying conditions. Establishing a diagnosis typically involves several consultations to complete history-taking, investigations, and follow-up reviews.
In general practice, ME/CFS is a clinical diagnosis based on:
- A detailed medical history and examination, including current symptoms and functional impact
- Standardised screening of ME/CFS symptom domains
- Investigation of symptom causes and identification of overlapping or co-existing conditions
There is currently no single diagnostic test for ME/CFS. Emerging investigations may assist in identifying patient subgroups and guiding targeted management; however, these are not yet validated as definitive diagnostic tools.
The main diagnostic steps include:
Step 1: Comprehensive History and Examination
Take a detailed medical history and conduct a physical examination to assess fatigue, identify potential causes, and evaluate for post-exertional symptom exacerbation.
Step 2: Routine Screening Investigations
Complete routine blood and urine tests to investigate causes of fatigue and exclude other medical conditions.
Step 3: Targeted Investigations
Order additional tests as indicated by personal history or previous results. These may assist in identifying clinical subgroups and informing later management.
Step 4: Mental Health Assessment
Where appropriate, exclude depression or other mental health conditions through brief discussion or a written/oral assessment tool.
Step 5: Symptom Review and ME/CFS Criteria
Once initial investigations are complete, reassess to identify key symptom domains to inform targeted management planning using the detailed ME/CFS symptom list.
Step 6: Specialist Referral
Where necessary refer to relevant specialists for disease-specific investigations or management of more complex presentations.
Step 7 – Early Intervention Classification
For patients with persistent fatigue of unclear cause, including post-viral or post-infection fatigue, consider a provisional classification of idiopathic chronic fatigue.
Early rest and pacing are important for all age groups and are critical for preventing long-term deterioration in young people and those who are severely affected.
Patient Preparation
Encourage patients, or parents/carers in the case of young people, to keep a symptom diary to track fluctuations, triggers, and activity–symptom relationships.
- For severe patients, carers may assist with symptom reporting.
- For young people, consider school timetables, extracurricular activities, and cognitive load when interpreting symptom patterns.
For more information:
- Clinical Care Guide: Managing ME/CFS, Long COVID & IACCs, First Edition, May 2025. Utah, USA: Bateman Horne Center
- Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Essentials of Diagnosis and Management (Bateman et al., 2021, Mayo Clinic Proceedings, 96(11):2861-2878) – open access.
- International ME/CFS Primer for General Practitioners, 2014
- Beyond ME/CFS: Report Guide for Clinicians, (GP Recommendations), Institute of Medicine, 2015 (20 pages
Further explanation of symptoms presenting
Primary Symptom
Post Exertional Malaise (PEM), the failure to recover after physical or mental activities. This is a substantial reduction to previous levels that significantly interferes with daily work and activities.
In the clinical assessment of ME/CFS, this unexplained Post Exertional Malaise, sometimes interpreted as fatigue, lasts > 6 months duration and is not the result of ongoing exertion and/or is not alleviated by rest.
Delays in diagnosis remain a major barrier to timely care. Australians with ME/CFS typically wait 2–5 years and often undergo multiple medical consultations before receiving a diagnosis (Emerge Australia, 2023). These prolonged delays contribute to avoidable disability, fragmented care, and increased long-term health-system costs.A 2024 South Australian study demonstrated that GP practice nurses can provide early-intervention screening and management using an adapted nurse-led Medicare Chronic Disease Management approach with standardised tools. This model enables patients to begin tailored management, prioritising pacing and energy management to prevent deterioration, while awaiting further investigations or specialist referrals (Bridges & Pathways, 2024).This approach also enables the early identification of people with severe or very severe ME/CFS, who require urgent, modified care. Standardised screening allows practice nurses and GPs to “red flag” patients who are housebound or significantly functionally impaired, ensuring priority follow-up, reduced sensory exposures, and rapid referral pathways. Early recognition of severe presentations is essential to prevent clinical deterioration and to support safe management within primary care.
Download Assessment Tools here
Additional Symptoms important in diagnosis and management include:
- Neuro-cognitive dysfunction – significant impairment of short-term memory or ability to concentrate
- Sleep disorders – unrefreshing sleep or changes in sleep patterns
- Orthostatic intolerance including reduced mobility
- Autonomic manifestations – light-headedness, heart palpitations, shortness of breath
- Gastro-intestinal symptoms including irritable bowel or nausea
- Pain – muscle pain and weakness, joint pain
- Headaches of a new pattern or severity
- Immune manifestations – flu-like symptoms, sore throat and/or tender cervical or axillary nodes
- Other sensitivities including food, light, noise, smells and/or temperature
- Sensitivities to medication
- Neuro-endocrine manifestations – change in body temperature, or intolerance of heat or cold and stress
Patient information sheets on diagnosis are available download Patient Handouts here
- What is ME/CFS? Part A
- What is ME/CFS? Part B
- Understanding the Diagnostic Process
While waiting for a diagnosis patients are encouraged to:
- Focus on wellness and healing
- Slow down and allow your body to rest and heal
- Stop pushing through, as ME/CFS and many chronic conditions are sensitive to stress
- Record events leading up to your illness
- Record the changes in your symptoms and activity levels, to guide management
- Keep a diary of everything you try, or anything that changes – including treatments and lifestyle adjustments
- Be informed, be empowered